
Uncategorized
Retatrutide Masterclass: Clinical Trials, Mechanism of Action, Weight Loss Data and What the Research Really Shows

May
etatrutide is one of the most discussed names in metabolic research because it was built to do something more ambitious than earlier incretin-based compounds. Instead of acting on one pathway, or even two, retatrutide is designed as a triple hormone receptor agonist that activates the receptors for GLP-1, GIP, and glucagon. That three-part mechanism is the reason researchers have watched it so closely, and it is also the reason it continues to stand out in obesity and metabolic trial data. (lilly.com)
What has driven so much interest is not just that retatrutide produced large average body-weight reductions in early studies. It is that the evidence suggests a broader metabolic effect: weight loss, glycaemic improvement, changes in triglycerides, changes in liver fat, and a mechanism that may help explain why the numbers were so strong. In other words, this is not simply another peptide being discussed because it is “new.” It is being studied seriously because the published data already showed a profile that looked unusually powerful for an investigational compound. (New England Journal of Medicine)
If you are researching Retatrutide UK, buy retatrutide UK, retatrutide trials, retatrutide mechanism, or retatrutide vs tirzepatide, this is the kind of guide that should give you a real understanding of what the compound is, why the data matter, and what the current evidence actually says. The goal here is not hype. It is clarity. (lilly.com)
What Is Retatrutide?
Retatrutide, also known by the development code LY3437943, is an investigational once-weekly injectable peptide being developed by Eli Lilly. Lilly describes it as a triple hormone receptor agonist because one molecule is designed to activate the body’s receptors for GIP, GLP-1, and glucagon. In current development, it is being studied across obesity, overweight with related conditions, type 2 diabetes, and several broader cardiometabolic and liver-related settings. (lilly.com)
That single sentence already explains why retatrutide is different from the compounds it is often compared with. Semaglutide is built around GLP-1 receptor agonism. Tirzepatide is built around dual agonism at GLP-1 and GIP. Retatrutide adds a third target: glucagon. That does not automatically guarantee better outcomes in every setting, but it does create a more expansive metabolic design, and that three-pathway design is central to understanding the trial results that followed. (lilly.com)
How Retatrutide Works: Why the Triple Agonist Mechanism Matters
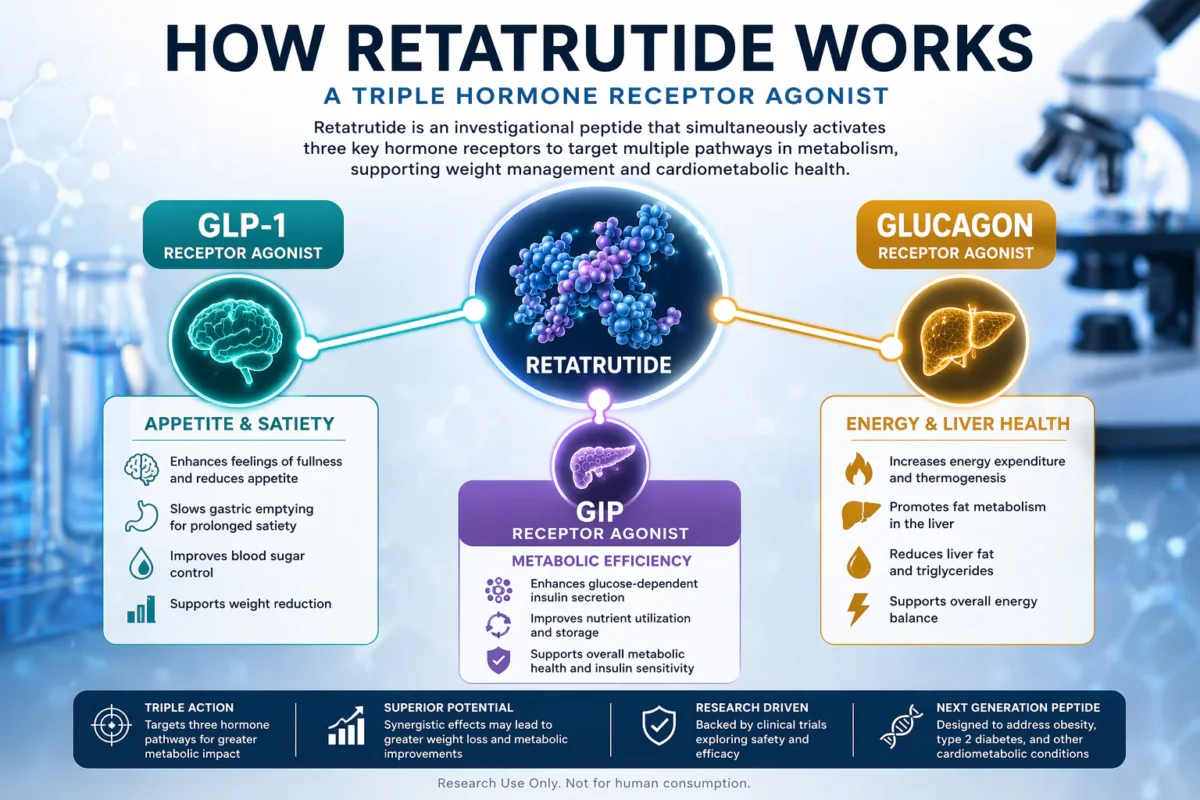
- GLP-1 → appetite and satiety
- GIP → metabolic signalling and insulin response
- Glucagon → energy expenditure and liver-fat metabolism
Why here: This is the first major “teaching” section, so a visual helps the reader understand the mechanism before you move into trial data.
To understand why retatrutide has drawn so much attention, it helps to break the mechanism down into plain English. GLP-1 receptor agonism is most closely associated with appetite regulation, delayed gastric emptying, and improved glucose handling. GIP receptor agonism appears to complement incretin signalling and may improve metabolic response. The unusual part is glucagon receptor agonism, which researchers think may support higher energy expenditure and may also influence liver-fat metabolism. Put together, the theory is simple: retatrutide may reduce energy intake, improve nutrient handling, and increase energy output at the same time. (lilly.com)
This is why people often describe retatrutide as a “next-generation” peptide. It is not just doing more of the same thing. It is built around a broader metabolic strategy. The obesity phase 2 trial and the later MASLD substudy both fit that idea. In obesity, retatrutide produced substantial dose-related body-weight changes. In the liver-fat substudy, it was associated with very large relative reductions in liver fat, particularly at the higher doses. These two findings make more sense when viewed through the triple-agonist mechanism rather than through appetite suppression alone. (New England Journal of Medicine)
The Retatrutide Obesity Trial That Changed Everything
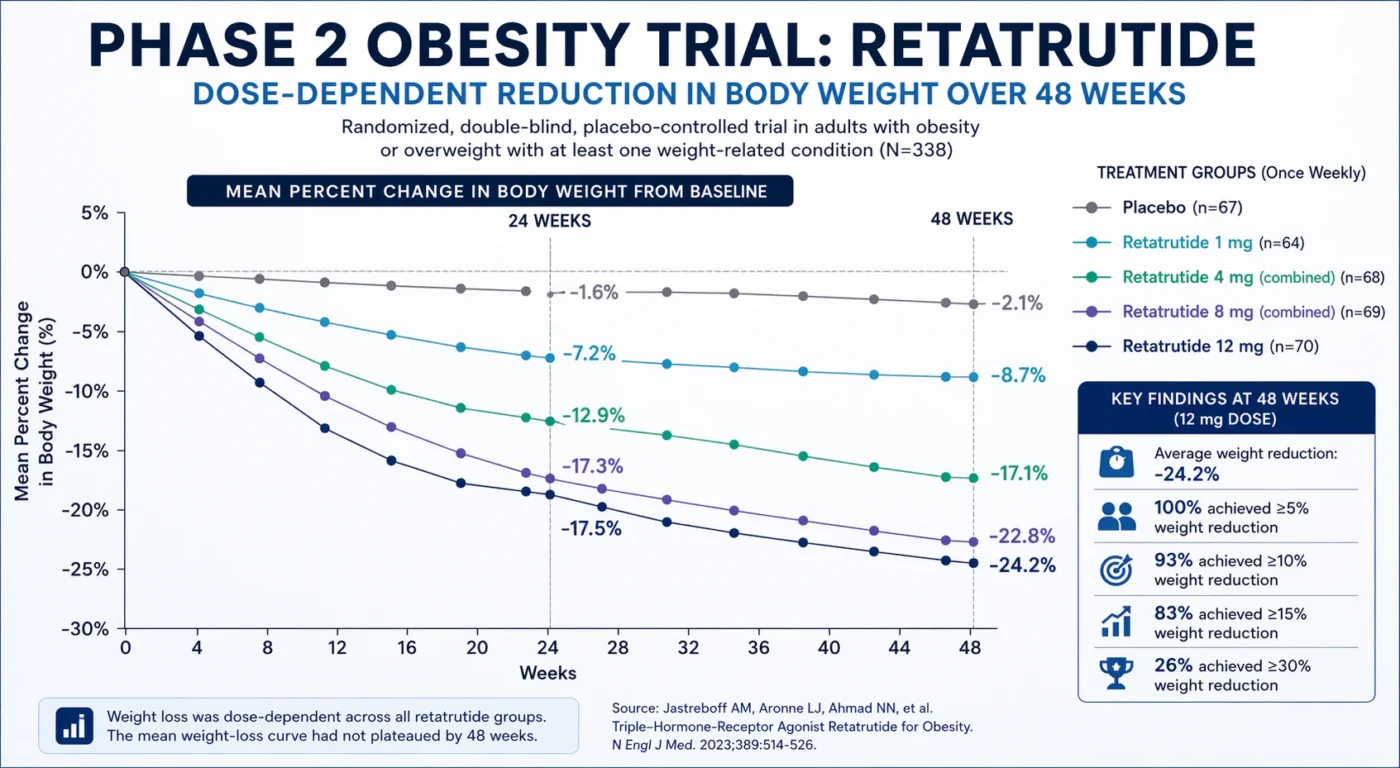
The phase 2 obesity study is the paper that made retatrutide impossible to ignore. Published in The New England Journal of Medicine, it was a double-blind, randomized, placebo-controlled trial in 338 adults with obesity, or overweight plus at least one weight-related condition. Participants received once-weekly retatrutide across different dose-escalation strategies for 48 weeks, with the primary endpoint focused on percentage change in body weight at 24 weeks. (New England Journal of Medicine)
The headline numbers are the reason this study is quoted so often. At 24 weeks, least-squares mean body-weight change was -7.2% at 1 mg, -12.9% in the combined 4 mg groups, -17.3% in the combined 8 mg groups, and -17.5% at 12 mg, versus -1.6% with placebo. By 48 weeks, those changes were reported as -8.7%, -17.1%, -22.8%, and -24.2% respectively, compared with -2.1% for placebo. Those are unusually large effects for a mid-stage obesity trial, and they are the main reason retatrutide became one of the most talked-about compounds in this space. (New England Journal of Medicine)
The numbers become even more striking when you look at weight-loss categories rather than simple averages. In the 12 mg group at 48 weeks, the NEJM paper reported that 100% of participants achieved at least 5% weight reduction, 93% achieved at least 10%, 83% achieved at least 15%, and 26% achieved 30% or more. Those are the kinds of figures that move a compound from “promising” to “seriously watched.” (New England Journal of Medicine)
Another detail from the same paper matters a great deal: the weight-loss curves had not clearly plateaued by the end of the 48-week treatment period. In simple terms, participants were still trending downward. That is one of the reasons later phase 3 development has been watched so closely. When a compound produces strong numbers and the curve still looks active at the end of the observation window, researchers immediately want to know what happens over longer durations. (New England Journal of Medicine)
What the Obesity Trial Suggests Beyond Weight Loss
One of the most important points in the NEJM paper is that retatrutide was not only associated with reductions in body weight. The study also reported improvements in waist circumference, blood pressure, glycated haemoglobin, fasting glucose, insulin, and multiple lipid-related measures as exploratory endpoints. In participants with prediabetes at baseline, 72% in the retatrutide groups had returned to normoglycaemia by week 48, versus 22% in placebo. (New England Journal of Medicine)
This matters because it changes how the compound should be discussed. If a molecule only produced body-weight change, it would still be interesting. But a pattern that also touches glucose regulation, waist size, triglycerides, and broader cardiometabolic markers suggests a more complete metabolic effect. That is why retatrutide is often discussed as part of the bigger future of obesity and metabolic medicine, not just as a “research fat-loss peptide.” (New England Journal of Medicine)
product links here:
- 20mg Retatrutide Pen (VLS)
- 30mg Retatrutide (Remedium Research)
- 40mg Retatrutide (Synedica) (Buy Retatrutide Online UK)
Researchers interested in different Retatrutide UK formats can also explore your current research listings, including the 20mg Retatrutide Pen (VLS), 30mg Retatrutide (Remedium Research), and 40mg Retatrutide (Synedica). (Buy Retatrutide Online UK)
Retatrutide in Type 2 Diabetes: Why the Diabetes Data Matter
Retatrutide also showed a strong signal in type 2 diabetes. The phase 2 trial published in The Lancet concluded that retatrutide delivered clinically meaningful improvements in glycaemic control together with robust reductions in body weight, with a safety profile broadly consistent with what is known from incretin-based therapies. (The Lancet)
That finding matters more than many readers realise. Some compounds perform strongly in obesity populations without diabetes, but the effect weakens once type 2 diabetes enters the picture. Retatrutide did not disappear in that setting. It still showed meaningful glucose-lowering and meaningful body-weight change, which supports the idea that it is acting as a broader metabolic compound rather than as a narrow one-trick intervention. (The Lancet)
Lilly’s March 2026 announcement on TRANSCEND-T2D-1, described as the first phase 3 diabetes trial for retatrutide, adds to that story. Lilly reported average A1C reductions of 1.7% to 2.0% across doses at 40 weeks, and average body-weight reduction of 16.8% in the 12 mg group. Lilly also said there was no weight-loss plateau observed through 40 weeks. Those are company-reported topline results rather than a full peer-reviewed publication, but they suggest that the phase 2 signal in diabetes may be continuing into phase 3. (Eli Lilly and Company)
internal comparison links here:
- 20mg Tirzepatide (VLS)
- 50mg Tirzepatide (VioGen)
- Retatrutide vs Tirzepatide: Key Differences Explained for Research Use (Buy Retatrutide Online UK)
For researchers comparing triple-agonist and dual-agonist pathways, it is useful to review both your 20mg Tirzepatide (VLS) and 50mg Tirzepatide (VioGen) Retatrutide vs Tirzepatide guide. (Buy Retatrutide Online UK)
Body Composition: Was Retatrutide Mostly Reducing Fat?
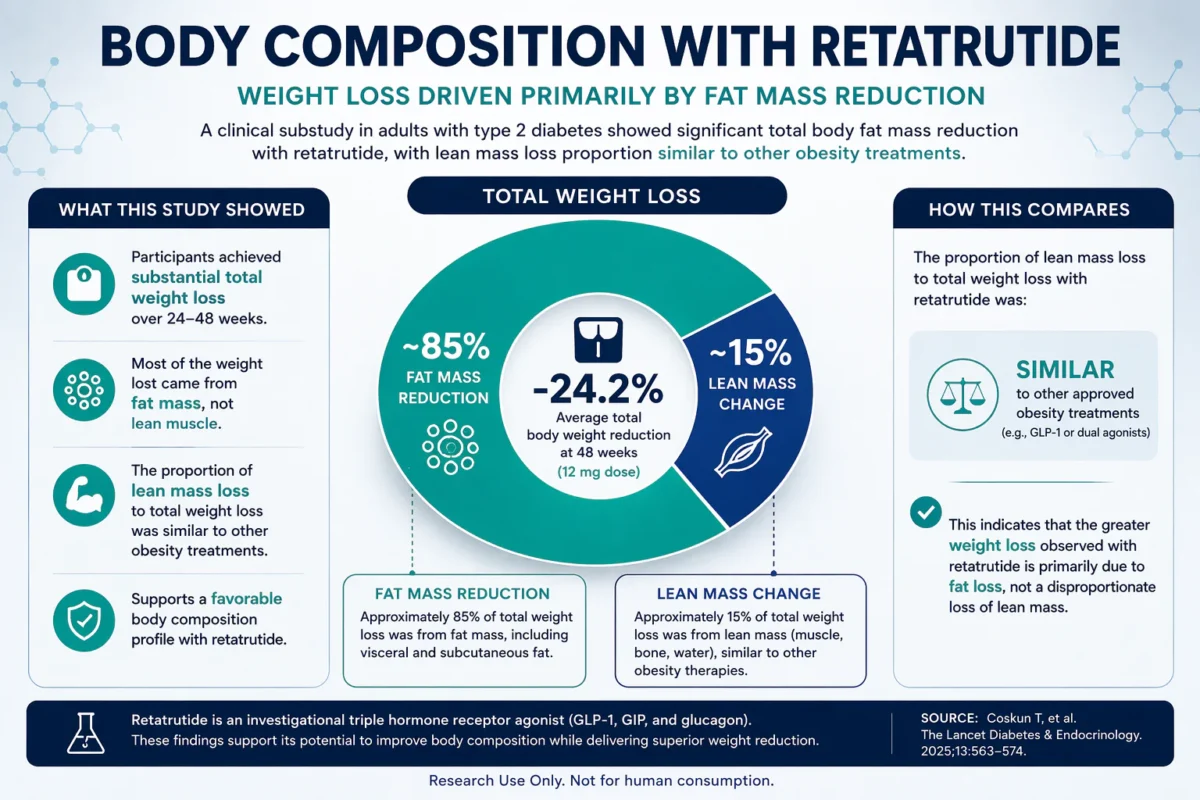
One common criticism of very strong body-weight data is the concern that the weight lost may not be predominantly fat. That is why the later body-composition substudy matters. In 2025, The Lancet Diabetes & Endocrinology reported that retatrutide significantly improved total body fat mass reduction compared with placebo and dulaglutide in adults with type 2 diabetes, and that the proportion of lean mass loss to total weight loss was similar to what has been seen with other obesity treatments. (The Lancet)
That does not mean lean mass should be ignored. It means the available evidence does not suggest that retatrutide’s larger weight-loss effect is being driven by an unusually poor body-composition tradeoff. For readers who want a more mature understanding of the evidence, this is one of the most useful details to include because it answers a question sophisticated readers often ask. (PubMed)
BODY COMPOSITION VISUAL:
Liver Fat, MASLD and Why the Liver Data Are So Important
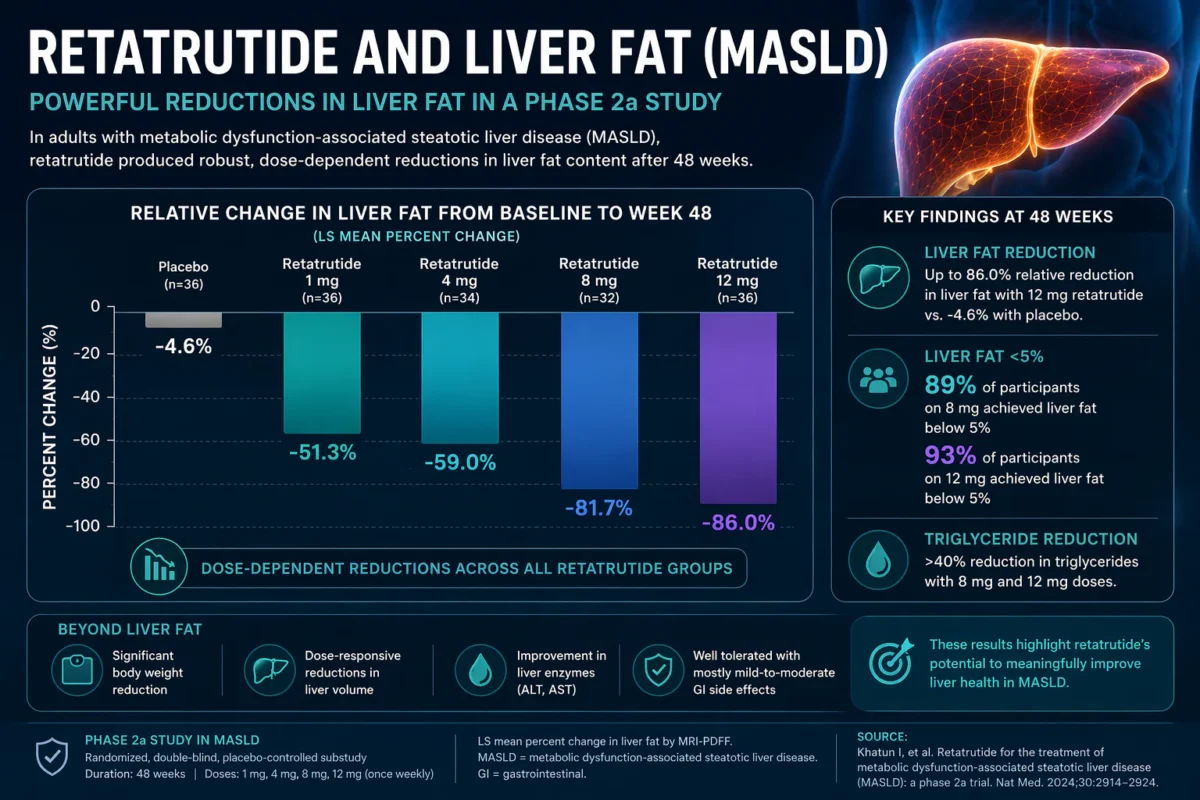
In a 2024 Nature Medicine phase 2a substudy of participants with metabolic dysfunction-associated steatotic liver disease (MASLD), retatrutide produced very large relative reductions in liver fat. At 48 weeks, relative liver-fat changes from baseline were -51.3%, -59.0%, -81.7%, and -86.0% for the 1 mg, 4 mg, 8 mg, and 12 mg doses respectively, compared with -4.6% for placebo. (Nature)
The same sub-study reported that with the 8 mg and 12 mg doses, total liver fat content below 5% was achieved by 89% and 93% of participants respectively at 48 weeks. It also showed significant reductions in body weight, dose-responsive reductions in liver volume, and triglyceride reductions of more than 40% with the 8 mg and 12 mg doses after 48 weeks. (Nature)
This is one of the strongest examples of why glucagon receptor agonism matters in the retatrutide story. Appetite reduction alone does not fully explain data like this. The liver-fat findings fit much better with the idea that retatrutide is working across several metabolic layers at once: appetite, nutrient handling, lipid metabolism, insulin sensitivity, and liver-fat biology. That is why the liver data are so valuable from a scientific point of view, and why they deserve a major section in a genuine “retatrutide masterclass.” (Nature)
Lilly’s own medical information also notes that retatrutide is now being studied in a phase 3 liver-outcomes programme called SYNERGY-Outcomes, designed to assess retatrutide and tirzepatide in adults with high-risk MASLD. Lilly states the study plans to enroll about 4,500 adults and run for approximately 224 weeks, with an optional extension. That tells you how seriously the liver signal is being taken. (Lilly Medical)
LIVER FAT / MASLD GRAPHIC
Safety and Side Effects: What the Trials Reported
In the phase 2 obesity trial, the most common adverse events were gastrointestinal: nausea, diarrhea, vomiting, and constipation. These events were dose-related, occurred mainly during dose escalation, and were reported as mostly mild to moderate. The paper also noted that lower starting doses partly mitigated gastrointestinal events. (New England Journal of Medicine)
The NEJM paper also reported dose-dependent increases in heart rate that peaked at around 24 weeks and declined thereafter. Serious adverse events occurred at similar frequencies in the retatrutide and placebo groups in that study, though the paper did note one serious event of acute pancreatitis in the context of asymptomatic amylase and lipase increases. That does not erase the strength of the efficacy signal, but it is an important part of an honest summary of the evidence. (New England Journal of Medicine)
The MASLD sub-study reported a broadly similar safety picture, with transient, mostly mild-to-moderate gastrointestinal events being the most frequent adverse events, especially during dose escalation and more often in the higher-dose groups. (Nature)
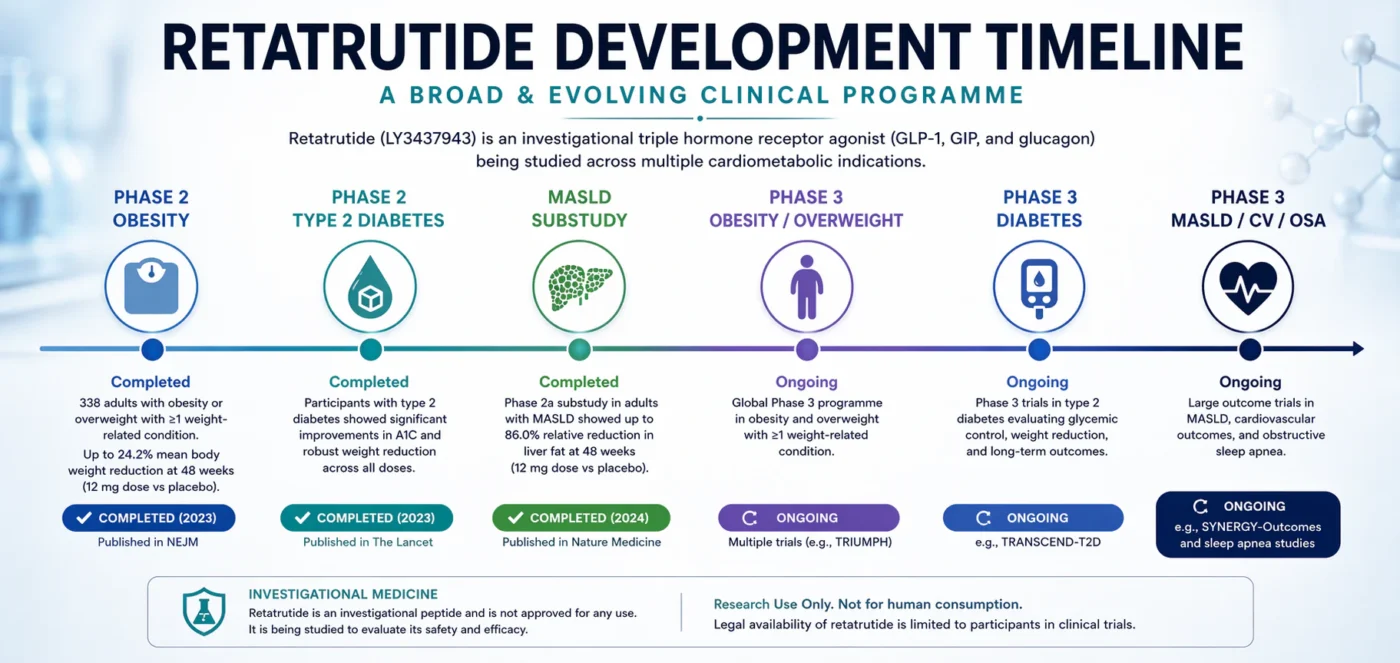
Where Retatrutide Is Now: Phase 3 Development
Retatrutide is still investigational, but by 2026 it is no longer just a phase 2 story. Lilly states that the compound is in several phase 3 clinical trials for obesity and overweight with at least one weight-related condition, type 2 diabetes, knee osteoarthritis, obstructive sleep apnea, chronic low back pain, cardiovascular and renal outcomes, and MASLD. ClinicalTrials.gov and Lilly trial listings confirm major ongoing work in obesity/overweight master protocols and in obesity with established cardiovascular disease. (Eli Lilly and Company)
That development footprint matters because it shows how Lilly sees retatrutide: not as a narrow one-indication candidate, but as a broad cardiometabolic molecule with multiple possible applications. It also means that the retatrutide story is still evolving. The strongest published data so far come from phase 2 obesity, phase 2 diabetes, and the MASLD substudy. The next big wave of evidence will come from larger and longer phase 3 studies. (New England Journal of Medicine)
DEVELOPMENT TIMELINE
Final Verdict: Why Retatrutide Matters
Retatrutide matters because it combines an ambitious mechanism with some of the most striking mid-stage metabolic trial data seen in recent years. The phase 2 obesity study showed up to 24.2% average body-weight reduction at 48 weeks. The type 2 diabetes study showed meaningful HbA1c and body-weight improvements. The body-composition substudy suggested that the greater weight loss was still largely driven by fat mass reduction. The MASLD data showed major effects on liver fat that deepen the scientific rationale behind the compound. (New England Journal of Medicine)
That does not mean the story is finished. Retatrutide is still investigational, still unapproved, and still awaiting the kind of full phase 3 published evidence that ultimately determines how durable and safe a treatment looks at scale. But based on what is already in the literature, it is completely fair to say that retatrutide is one of the most important compounds currently being studied in obesity and metabolic research. (lilly.com)
For readers exploring Retatrutide UK and research-use peptide options, the best way to view the compound is not as hype, but as a serious investigational peptide with a mechanism and evidence base that are both broader than most quick summaries suggest. That is exactly why it deserves a proper masterclass. (lilly.com)
Research-Use Disclaimer
Retatrutide is an investigational research compound. It has not been approved for general medical use and is not for human consumption. This content is provided for research and educational purposes only. Lilly states that retatrutide is legally available only to participants in its clinical trials. (lilly.com)
Internal Links – Products
- 20mg Retatrutide Pen (VLS) (Buy Retatrutide Online UK)
- 30mg Retatrutide (Remedium Research) (Buy Retatrutide Online UK)
- 40mg Retatrutide (Synedica) (Buy Retatrutide Online UK)
- 20mg Tirzepatide (VLS) (Buy Retatrutide Online UK)
- 50mg Tirzepatide (VioGen) (Buy Retatrutide Online UK)
- Retatrutide vs Tirzepatide: Key Differences Explained for Research Use (Buy Retatrutide Online UK)
- How Long Does Retatrutide Take to Work? if that is your live slug, or your equivalent live post. (Buy Retatrutide Online UK)